Please meet Jason*. He loves sports. As I write, I can picture him telling me blow-by-blow how he made the winning shot in his last basketball game. This was an experience I had with Jason many times.

Source: http://www.tmp-m.org
Jason is a talented skateboarder and basketball player, and he enjoys football and soccer, too. His favorite video game is Madden. Jason is also pretty good with the drums. He plays on some Sundays at his church and in his uncle’s band. Jason has told me that school is not his favorite thing, but the classes he enjoys are gym, math, and science. He “hates” social studies and finds language arts challenging, sometimes. Jason wants to become a police officer when he grows up. I have heard his maternal uncle say often, “he is a great kid.” His mother has described him as a “good big brother, [and] helpful with his little sister.” He picks his sister up from school at the end of the day and makes sure she settles in with a snack and one of her favorite cartoons before she has to do her homework. Jason has told me how important it is for him to be a “good big brother to his sister, like his uncle is to him.” Jason’s biological father died in a tragic car accident when Jason was eight years old. His mother and uncle have shared with me how Jason is serious about being a positive role model to his sister.
You may be thinking that this is a dream kid! How did he come to the place where he would be in need of in-home behavioral health services?
The answer is in the way Jason was presented to me through a referral.
“A 13 year old Black male who lives with his single mother and younger sister, 7 years old. He is diagnosed with Attention Deficit Hyperactivity Disorder (ADHD) and Oppositional Defiant Disorder (ODD). He is defiant towards household and school rules and directives given by his mother and teachers. Jason’s mother is having a difficult time managing Jason’s behaviors because he is argumentative and becomes hostile with her when she tells him no and disagrees with him.”
It sounds like two different boys.
After a few sessions with Jason, his mother, and, occasionally, his uncle, I got to see pretty quickly that there was more to Jason than the description presented to me. He was more than the labels and diagnoses used to describe him.

There was one session, when I arrived at the home after working with the family for a few months. I entered the house through the backdoor and directly into their kitchen. As I walked in, Jason and his mother were in the midst of a disagreement. I heard their voices when I was on the back porch. Jason’s mom said, “Jason you have got to listen and stop fighting everything. You are the poster child for ODD.” Jason replied, “I’m not ODD!” I knocked on the door and Jason’s mother opened the door. She said, “Come on in Ms. Tawanda. Maybe you can get him to understand.”
I acknowledged the mother with a head nod. I gave an empathic look at Jason and said hello. His head was down and he was looking in the direction of the family’s living room away from the backdoor.
The mother and Jason had just come home, about 20 minutes before I arrived from a meeting at the school. It was another meeting with Jason’s school case manager and two of his teachers who reported Jason was being “disruptive, disrespectful and giving them a hard time [and] refusing to complete certain activities and constantly asking questions.”
After I met with Jason and his mother together, I talked to Jason alone. It took him a few minutes, but after a mini-break where he got something to drink and a snack, he was his lively self again. Jason shared with me his perspective on the meeting and the complaints made: “they don’t get it. If they were able to say things in a clear way, I would not have to ask a million questions, and I am not going to do assignments that make no sense.” I listened closely to Jason’s complaints and we explored whether his approach was helpful or hindering him in meeting his goals. We brainstormed together some alternative approaches that he could try. I asked Jason about the moment when I had arrived and he was not talking. He had looked shut down. Jason didn’t respond immediately. Then, he said, “I hate when my mom says to me, its my ADHD or ODD. It’s not mine. I am not a disorder. I am Jason.”
Source: www.embracenl.org
This is a small peek into Jason’s world, his struggle with the labels used in our society to describe his behaviors, some of his ways of relating to others and how others experience and treat him.
***********************************************************************
Source: http://www.helpyourteennow.com
A Closer Look at Oppositional Defiant Disorder
Oppositional Defiant Disorder (ODD) is a diagnose in the category of disruptive behavior disorders in the American Psychiatric Association’s (APA) of the Diagnostic and Statistical Manual of Mental Disorders (DSM). The DSM is “a categorical classification that divides mental disorders into types based on criteria sets with defining features. This naming of categories is the traditional method of organizing and transmitting information in everyday life and has been the fundamental approach used in all systems of medical diagnosis.” (APA, 2000, p. xxxi,)
The DSM has been in existence since 1952 with the release of DSM-I. We are now utilizing the fifth edition of the DSM-5, published in 2013. In the DSM-5, the group that the diagnosis of ODD has been situated in is the Disruptive, Impulse-Control and Conduct Disorders group. The essential features of ODD, as described in DSM-5, is a pattern of angry/irritable mood, argumentative/defiant behavior, or vindictiveness lasting at least six months as evidenced by at least four symptoms from any of the three categories and exhibited during interaction with at least one person who is not a sibling (p 462, APA, 2013).
Source: http://www.psychologytoday.com
ODD was not always called ODD, In DSM-II, the diagnosed that resembled our present ODD was situated in the category of Behavioral Disorders of Childhood and Adolescence. The disorders that made up that category consisted of hyperkinetic reaction, withdrawing reaction, overanxious reaction, runaway reaction, unsocialized aggressive reaction, and group delinquent reaction. The one that closely resembles our present ODD with some features of our present Conduct Disorder is Unsocialized Aggressive Reaction (308.4) which is “characterized by overt or covert hostile disobedience, quarrelsomeness, physical and verbal aggressiveness, vengefulness and destructiveness. Temper tantrums, solitary stealing, lying, and hostile teasing of other children are common (APA, 1968, p. 51).
In DSM-III ODD was revealed, and “the essential feature of this disorder is a pattern of negativistic, hostile and defiant behavior without serious violations of basic rights of others that are seen in Conduct Disorder” (APA, 1987, p, 56) As you can see the name of the disorder, its features and its organization has changed from DSM-II to DSM-5.
Stringaris and Goodman (2009), based on research findings that ODD may encompass symptoms that go beyond what is expected as typical disruptive disorders, claim oppositionality is composed of three dimensions: irritable—strongly connected to emotional disorders, headstrong—connected with ADHD, and hurtful (linked to aggressive symptoms in CD). You can see the details of this breakdown in the essential features for ODD in DSM-5.
ODD is one disorder that can stand alone, but typically co-occurs with ADHD and has a wide range of association with other disorders, such as conduct disorder, anxiety, depression, and obsessive-compulsive disorder (Drabick & Gadow, 2012; Stringaris & Goodman, 2009; and Krieger, Polanxzyk, et.al, 2013).
I prefer the explanations and definitions in the DSM-IV-TR for mental disorder, I find the the language that is utilized is easy to understand. According to DSM-IV-TR, “each of the mental disorders is conceptualized as a clinically significant behavioral or psychological syndrome or pattern that occurs in a individual and that is associated with present distress…disability… or with a significantly increased risk of suffering death, pain, disability or an important loss of freedom…Whatever its original cause, it must currently be considered a manifestation of a behavioral, psychological, or biological dysfunction in the individual (APA, 2000, p. xxxi).”
One of the areas I feel challenged by and consider a limitation with of the DSM is that the problem is located solely in the individual. There are only a few diagnoses in the DSM-5 that locate the problem outside of the individual which belong to the Trauma and Stressor Related Disorders, like Post-traumatic Stress Disorder (PTSD), Reactive Attachment Disorder, Adjustment Disorders, etc. According to the DSM-5 “the traumatic or stressful event is listed explicitly as a diagnostic criterion” ( APA, 2013, p. 265).
Source: http://www.pbs.org
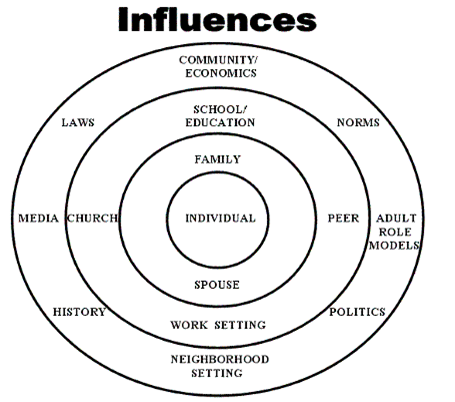
In social work, we privilege the holistic approach by looking at individuals, the connections between them and others, and the many environments they inhabit. Social workers work with individuals, families, groups and communities on micro, mezzo and macro levels, which gives them the flexibility to identify and work with problems and issues that arise between people and between people and their environments, including culture and society.
But there is a need for categorizing, mental disorders, and the DSM.
According to the DSM-5, “reliable diagnoses are essential for guiding treatment and recommendations, identifying prevalence rates for mental health service planning, identifying patient groups for clinical and basic research, and documenting important public health information such as morbidity and mortality rates. As the understanding of mental disorders and their treatments has evolved, medical, scientific, and clinical professionals have focused on the characteristics of specific disorders and their implications for treatment and research.” (2013, p.5)
Allen Frances, MD, chair of DSM-IV Taskforce, stated in his book, Saving Normal (2013), reliability and validity is important in defining disorders. “Reliability means agreement and consistency—will different clinicians seeing the same patient arrive at the same diagnosis. Validity means truth—will the diagnosis tell you what you want to know” (p. 25).
He went on to claim DSM criteria are simple and “a catalog only of what is most surface and common in mental disorders”. The rich diversity of individual difference and experiences are “obscured” in DSM definitions. The “DSM definitions do not include personal and contextual factors…DSM has to stay simple”(Frances, 2013, pp. 25–26). Yet, it has become so influential in our field.
This is my concern: the DSM is too simple, loses personal and contextual factors, and is influential. I value my MSW education and clinical training as a social worker for giving me the holistic perspective, including personal and contextual factors. I feel fortunate for my DSW education, which taught me to identify my theoretical and value commitments, not to follow blindly reductionist models, to use a trandisciplinary approach, and to complicate ideas rather than simplify them. This could be one of the reasons why social workers are the largest group of providers of mental and behavioral healthcare services in the United States.
Let’s go back to Jason. Remember that he was introduced to me on the basis of his diagnoses and behaviors, with minimal information given to me about his contextual factors and nothing about his strengths and positive qualities. Like Allen Frances (2013) states, the DSM is influential. Diagnoses, along with the theoretical orientation, inform what a clinical social worker pays attention to, her attitude towards an individual or family, and her selection of interventions. If the DSM were the sole authority I utilized, I would have never come to see Jason as more than his behavior or the labels ascribed to him—that is, to see and experience Jason as a person.
We cannot drink the Kool-Aid. This includes parents, too.
“We live in a world of ideas” Gregory Bateson
According to Ian Hacking (1999), ideas and objects interact, which means that the ways of classifying human beings interact with the human being who are being classified. This was evident in Jason’s Mother’s words to him, “you are a poster child for ODD,” as well as his reaction.
Jason illustrates Hacking’s (1999) idea that “people think of themselves as a kind … all our acts are under descriptions, and the acts that are open to us depend, in a purely formal way, on the descriptions available to us … people are aware of what is said about them, thought of them and done to them” (p. 31). The DSM provides our society with descriptions. Is this why it is so influential?
Some of David Sparti’s (2001) ideas in his article, Making Up People, echoes Ian Hacking idea of “interactive kinds”, which emphasizes the power of naming and looping effect between categories and identities having a reciprocal formed relationship.
What we name our children doesn’t stop with their legal name; rather, that’s just the beginning. The names and labels that are affixed to our children, including diagnoses, get internalized and become who they are and how others may see and treat them. It is how we “make up people” and people come to see themselves as certain “kinds” of persons.
For a good example of how labels and disorders are “interactive kinds,” let’s look back in time. Have you heard of Dr. Samuel A. Cartwright, a physician from the early 1850s?
One of his contributions to medicine is the creation of Drapetomania.
Source:www.mostlyodd.com
He claimed to have discovered a new disease, which he called Drapetomania, and he published his findings in the New Orleans Medical and Surgical Journal. He claimed that the runaway behavior of African-American slaves was a disease that could be prevented. He described how slaves were like children and loved to be constrained by authority. He gave strategies for slave masters to utilize to prevent runaway behaviors.
.

The runaway slaves were demonstrating defiance and rebellion. Dr. Cartwright classified their behaviors as a disorder. Demonstrating defiance and rebellion to an oppressor and oppressive system, a way of life like slavery—is that a disorder? I ask: from whose vantage point is it a disorder? The slave master or the person trapped in slavery and subjugated? Drapetomania is not valid today, and I dare to say, it was not valid in the past. Yet, it was utilized to name, relate, and treat a person and the behavior of slaves who were running away and seeking freedom.

Source: http://www.davidmcelroy.org
The DSM is one idea and it has its place, but its not the absolute and only way to categorize human experience.
Within the DSM, ideas are included, excluded, introduced and than taken out. Homosexuality was once considered a mental disorder and listed in the DSM under sexual deviance. It was removed in DSM III-R.
Source: http://www.1bp.blogspot.com
Is oppositional defiant disorder really valid?
Will oppositional defiant disorder one day be removed from the DSM?
***********************************************************************
In DSM-IV-TR (2000), in the description of ODD, the creators wrote, oppositional behaviors are a typical feature of certain developmental states (e.g, early childhood and adolescence). A diagnosis of ODD should be considered only if the behaviors occur more frequently and intensity is extreme with more severe consequences than what is typically observed in peers with comparable developmental stages. The emergence of new oppositional attitudes and behavior may be due to the process of normal individuation.
My claim connects to this idea in DSM-IV-TR that opposition is a typical part of adolescent development. I believe it needs to be seen on a continuum. Oppositionality in adolescence needs not to be feared or squashed. Opposition in adolescence is experienced and constructed relationally. It presents as a relational challenge and needs relational interventions. Adolescents need guidance, mentoring, and support to understand, express, and utilize opposition and defiance constructively. A non-blaming and strength-based approach: opposition as advocacy and assertion of power in relationships.
Nancy Nyquist Potter wrestles in similar ways I do with opposition with defiance in her article entitled, Mad, bad or virtuous? The moral, cultural and pathologizing feature of defiance. Potter (2011), brings attention to how “defiance is sometimes treated as a behavior that needs to be punished or diagnosed especially when it is expressed by the subjugated” . (p. 24)
Drapetomania. Adolescents.
Potter (2011) defines “defiance as a response to authority, specifically authoritative bodies use of power…belonging to a cluster of actions that include dissent, resistance, and civil disobedience. A defiant action is in your face, but it can be quiet as well” . (p.25) The defiant attitude and act is one of passion, possibly anger and commitment and can come across disrespectfully.
Potter (2011) claims, “to engage authority directly is important because it requires oppressors to acknowledge that their authority is being challenged… “acts of civil disobedience make a moral claim on oppressors to recognize our humanity”. (p.27)
Adolescents who oppose a social norm, rule or standard with a defiant attitude in a “direct or quiet way”, is challenging authority and “making a claim to be seen, heard and their humanity acknowledged” (Potter, 2011). They want a different treatment.
Potter (2011) raises concerns about how “defiance is sometimes managed socially through medicalizing it”.
It comes up often in my talk with caregivers. They share with me how a teacher or counselor at school told them that their adolescent has ODD and suggest that medication is needed. I bear witness to the caregiver’s struggle with considering the possibility of putting their child on medication. A part of them feels and thinks that it is not right, and another part of them just wants the child to behave. They are torn.
Potter writes, “… if young African American boys are being diagnosed with ODD, they may begin to respond to their classification by exhibiting closer approximations to it. Even attempts to defy that classification serve to confirm it. The concern is that schools and other institutions are not merely identifying the existent mental disorder but are creating the condition under which the disorder thrives.” (2011, p.33)
This sounds like Jason’s situation. He does not feel heard and taken seriously for his insight or how he learns best. So, he speaks up in ways that he feels heard. He does not act like the “good student” who obeys, which gets him labeled by authority figures in the school, officially or unofficially, with ODD. He acts in ways to “defy the classification,” but, based on the social system of which he is a part, he cannot escape the conditions that exist, which create the need for him to express himself in this manner. As long as he is a part of this system, he will be categorized and treated as one who is to be controlled, which creates the never-ending cycle of interaction between Jason and adults in school and other settings in oppositional and defiant ways.
The challenge for social workers, caregivers, and other professionals working with adolescents is to keep in mind that the diagnoses given to adolescents are only describing some of their behaviors and not their entire person. We must be careful not to equate a person with their behavior or exclude their personal and contextual factors by “keeping it simple.”
Human beings are complex. Adolescents are complex.
The expression of opposition and defiance needs to be taken seriously by “recognizing the claim another is making on you, norms that you enforce, practices that benefit you but not the defier. Taking defiance seriously means that you are willing to consider the possibility that you are implicated in abusive powers and oppressive regime. It indicates that you recognize the full humanity of the communicator” (Potter, 2011, p. 41).
I will take it a step further: adults must acknowledge that they are in the privileged power position with regards to adolescents. Adults run the world and adolescents are in vulnerable positions. We have to take extra steps to be mindful and vigilant to ensure that we don’t drink the Kool-Aid, leaving our children alone to struggle with the labels used to control, interact, treat, and assign value in our society. We must hear them and create conditions that enable them to thrive. If we take this approach, we will see the numbers drop in adolescents with the label of ODD.
Please keep Jason’s experience in mind with adolescents in your life.
Opposition in adolescence is experienced and constructed relationally. It presents as a relational challenge and needs relational interventions.
*Please note the case study is a composite and youth’s name changed for confidentiality purposes.
References
American Psychiatric Association (1952). Diagnostic and Statistical Manual of Mental Disorders, 1st Edition, Washington, D.C.
American Psychiatric Association (1968). Diagnostic and Statistical Manual of Mental Disorders, 2nd Edition, Washington, D.C.
American Psychiatric Association (1987). Diagnostic and Statistical Manual of Mental Disorders, 3rd-R Edition, Washington, D.C.
American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental Disorders, 4th-TR Edition, Washington, D.C.
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Washington, D.C.
Drabick, D. A. G. & Gadow, K. D. (2012). Deconstructing Oppositional Defiant Disorder: Clinic-Based Evidence for and Anger/Irritability Phenotype. Journal of American Academy of Child and Adolescent Psychiatry. 51:4, 384-392
Frances, A. (2013). Saving Normal. New York, NY: Harper Collins Publishers
Hacking, I. (1999). The Social Construction of What? Harvard University Press: Cambridge, Massachusetts and London, England
Petitclere, A. & Tremblay, R. E. (2009). Childhood Disruptive Behaviors Disorders: Review of Their Origin, Development, and Prevention. The Canadian Journal of Psychiatry, 54, 222-231.
Potter, N. N. (2011). Mad, bad or virtuous? The moral, cultural and pathologizing features of defiance. Theory and Psychology, 22(1), 23-45.
Sparti, D. (2001). Making up People: On Some Looping Effects of the Human Kind–Instiutional Reflexivity or Social Control? European Journal of Social Theory. 4(3), 331-349
Stringaris, A. & Goodman, R. (2009). Longitudinal Outcome of Youth Oppositionality: Irritable, Headstrong and Hurtful Behaviors Have Distinctive Predictions. Journal of American Academy of Child Adolescent Psychiatry, 48:4, 404-412
Valle Krieger, F. & et.al. (2013). Dimensions of Oppositionality in a Brazilian Community Sample: Testing the DSM-5 Proposal and Etiological Links. Journal of American Academy of Child and Adolescent Psychiatry. 52:4, 389-400
